Introduction
According to the World Health Organization, currently, about 17 million children and adolescents, between 5 and 17 years of age, suffer from a serious psychological disorder that warrants specialized treatment. Anxiety disorders are common conditions in childhood and adolescence1, with a worldwide prevalence that ranges between 4% and 32% in the medical literature2. Anxiety is considered an unpleasant emotional state, in which the subject makes a cognitive evaluation of that situation that he perceives, as a threat, which has a strong link with negative thoughts3. In addition, his comorbidity with depression is calculated between 30% and 60%4,5. It is considered that between childhood and adolescence, anxiety precedes depression6.
The depression is a pathological alteration of the state of mind. The Diagnostic and Statistical Manual of Mental Disorders establishes that major depression can be re-cognized by clinical signs and symptoms such as: Depressive state, marked decrease in interest or pleasure, alterations in the sleep cycle, loss or gain of weight corporal, psychomotor alterations, fatigue or loss of energy, feelings of sadness, hopelessness, guilt, uselessness, anhedonia, cognitive deficit that affects motivation, attention, concentration and memory, irritability, nervousness, low self-esteem, and suicidal ideas7,8.
The World Health Organization classifies depression as the fourth leading cause of disability worldwide9, which also affects around 350 million people, with prevalence ranging between 3.3% and 21.4%10. Depression is more frequent in the female gender, with an index of 5.8%, while for men it is 2.5%8.
In a study conducted in Mexico by the National Institute of Mental Health, it was concluded that in children and adolescents from 6 to 17 years, more than 6% of them had suffered a depressive disorder in the past 6 months, more than 15% manifested some of the symptoms of a major depressive disorder and 3% of the adolescents presented dysthymia11.
Some factors that modify the appearance of depressive symptoms are gender differences, cognitive activity, attitude to stressful events, coping styles, sensitivity to psychosocial stress, hormonal biological changes associated with pubertal maturation, and dimorphisms in the brain development between childhood and adolescence12.
According to demographic statistics, by the year 2030, it is projected that 5,000 million people, about 60% of the world’s population, will live in urban areas. This predisposes to increase the risks for the population in case of a disaster. A large-scale earthquake affecting these areas has the potential to cause considerable material damage and death due to the high demographic index13.
Worldwide in recent years, the frequency of catastrophes due to earthquakes has increased, and as a consequence, the incidence of various behavioral disorders has increased such as: anxiety, depression, psychosomatic diseases, sleep disorders, phobias, and post-traumatic stress disorder (PTSD)14.
The prevalence for PTSD was determined between 4.5% and 95%, while for depression, it was 13.6% and 76%, in a study conducted in children surviving an earthquake15.
Some aspects that influence the presentation and severity of psychological symptoms after an earthquake are: age, gender, marital status, loss of a loved one, proximity to the epicenter, personal health, previous existence of mental health problems, and injuries suffered16.
It has been shown that children and adolescents face adversity and loss differently, In addition, the magnitude of the catastrophe, the level of development, the history of violence or neglect, social aspects, the community, family dynamics, and parental relationship also influence them16,17.
The vulnerability of children and adolescents survivors to earthquakes is manifested by the presence of more severe psychiatric and somatic symptoms, these include: Sleep interruption, nightmares, fears related to the traumatic event, excessive attachment to caregivers, separation anxiety, loss of previously acquired skills, hyperactivity, irritability, difficulty concentrating, panic attacks, generalized anxiety disorder (GAD), depression, psychosomatic problems, enuresis, and substance abuse18.
Mexico is in a region of high seismic activity, the population has been sensitized after the experience of the earthquakes of 1957, 1985, and 2017; the last two occurred by coincidence on the same day, September 19.
The earthquake of September 19, 1985, in Mexico, was considered one of the most devastating earthquakes of the decade of the 80s, caused more than 1500 collapsed buildings and official dates of at least 10,000 deaths, in an emergent way a massive program of mental health in which psychiatrists, psychologists, and social workers intervened19.
In a study carried out on medical students surviving at the 1985 earthquake in Mexico, 15.8% of the population reported psychological symptoms associated with the earthquake; students who suffered serious physical damages or the loss of a close relative, showed greater severity in the overt signs of psychological illness20.
In the earthquake of September 19, 2017, UNICEF reported 369 deaths, of which 29 were children; 184,000 damaged houses and 38 collapsed buildings. About 71% of the people affected by this earthquake were women from Mexico City, the municipalities most affected in Mexico City were Álvaro Obregón, Benito Juárez, Coyoacán, Tlalpan, Tláhuac, and Xochimilco17.
This work analyzes the results of the anxiety and depression tests, obtained through the psychological evaluation carried out in students from 3rd to 6th grade of basic education of a private school, 1 month after the September 2017 earthquake in Mexico City, which caused human losses in two schools close to the referred to in this paper.
Methodology
Type: analytical transverse. Earthquake location: On September 19, 2017, an earthquake of magnitude 7.1 was generated at 13:14:40 pm, located on the state boundary between the states of Puebla and Morelos, 12 km South-east of Axochiapan, Morelos and 120 km from the Mexico City. The coordinates of the epicenter were: Latitude 18.40 north and longitude 98.72 west, at a depth of 57 km. The expansion of seismic waves affected the south and center area of the country’s capital (Fig. 1).
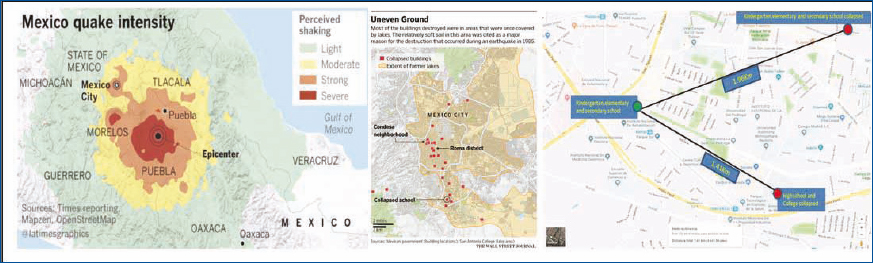
Figure 1. Region affected by the earthquake and location of collapsed school.
With the approval of the educational authorities, the informed consent form was sent to the parents to guarantee the participations of their children in the investigation. Sixty-two students from a private school in Mexico City were studied; this school is close to 2 of the schools that suffered major damages; one (basic level school) located 1.97 km away and the other (middle and upper level school), 1.50 km. Thirty-two female and 30 male subjects from 3rd to 6th grade of basic education were surveyed. The group of 3rd grade was formed by eighth students, four were girls and four boys; the group of fourth grade, by 12 students: Six girls and six boys. The fifth grade with 23 students: 14 girls and nine boys. Finally, sixth grade, with 19 students: eight girls and 11 boys. The informed consent form was delivered to the authorized students and the evaluation instruments were applied: Spence Children’s Anxiety Scale (SCAS) and the Child and Adolescent Depression Questionnaire (CADQ), both tests were done in a group manner, during class time, and ensuring anonymity.
Measures
Psychological tests: Two instruments were applied to evaluate the psychological profile of the students 30 days after the earthquake.
SCAS (Spence, 1997). It consists of 38 items related to anxiety symptoms with four Likert-type options: Never (0), sometimes (1), many times (2), and always (3). It also includes six positive items (false or distracting questions) that are not added to the value of the score. The 38 items are divided into six factors: “Panic Attack and Agoraphobia,” “Separation Anxiety Disorder,” “Social Phobia,” “Physical Fears,” “obsessive-compulsive disorder,” and “GAD.” It is qualified by the sum of the points obtained for each item. The higher the score means the greater of the anxiety.
CADQ consists of 27 questions, each answer correspond at one scale where 0 indicates “normality,” 1 “certain intensity,” and 2 “unequivocal presence” of a depressive symptom. When the higher score the intensity of depressive symptomatology is too. The responses 1, 3, 4, 6, 9, 12, 14, 17, 19, 20, 22, 23, 26, and 27 are evaluated 0, 1, and 2; while the rest with 2, 1, and 0. The recommended cutoff point for use as an assessment tool is 12 points, indicating that the child has psychological problems at 19 points or more, as an indicator of clear depressive symptoms.
Statistical analysis of our data was conducted using the SPSS software (SPSS 17). For the Spence Anxiety Scale, the Mann–Whitney test was applied, to find differences for each of the factors and between genders.
The Kruskal–Wallis test was used to determine the differences between the four scholar groups (3rd, 4th, 5th, and 6th grades), taking into account the six factors of the test. On the other hand, to analyze the results of the Spence test factors, a distribution of the data was established, assigning the percentiles in five levels of anxiety, according to the criteria proposed by Gaeta-González and Martínez-Otero21.
- First level, “Low,” from the 0 to 20 percentiles
- Second level, “Medium Low,” from the 21st to the 40 percentile
- Third level, “Medium,” from the 41st to the 60 percentiles
- Fourth level, “Medium High,” from the 61st to the 80 percentiles
- Fifth level, “High,” from the 81st to the 99 percentiles.
- With respect to the results of the questionnaire for depression, descriptive analysis and the χ2 test were applied.
This study is limited to the private schools in the affected zone where the study was conducted, included in the sample. Therefore, the results were evaluated in this context.
Results
We analyzed the results obtained in the groups from 3rd to 6th grade of primary school with the Spence test to assess anxiety.
Taking into account the total sample of students at the surveyed primary school (n = 62, of all school grades), there was a statistically significant difference (p = 0.012, p < 0.05) in the scores, when comparing them by gender (female, 50.65 and male, 41.16), using the Mann–Whitney test.
It was observed that in all school grades, the score was always higher in the female gender although without finding significant differences. The highest score by gender was obtained in the girls of the fourth grade (53.66), while the lowest score was obtained in the children of the fifth grade (38.88). With reference to the average total by grade level, the scores were simi-lar, although the highest values are observed in the groups of fourth (46.66) and sixth (46.57).
The group with less anxiety, according to their score (44.87) was the third grade, while the most anxious was the fourth grade (with 53.66).
Data were analyzed for the six factors that make up the Spence test, using the Mann–Whitney test to compare them between genders, finding statistically significant differences in three of the six factors: for “Panic attack and agoraphobia” there was significant difference in the factor total (p = 0.020). For “Separation Anxiety Disorder,” there was a significant difference in the sixth grade (p = 0.031) and in the total factor (p = 0.001). In “Physical Fears,” a significant difference was found in the sixth grade (p = 0.031) and in the total factor (p = 0.005) (Table 1). In the remaining factors (“social phobia,” “obsessive-compulsive disorder,” and “GAD”), no significant differences were found (Table 1).
Table 1. Significant differences between genders by factors
| Factors | Total | Female | Male | Diff. (p < 0.05) |
|---|---|---|---|---|
| Panic attacks and agoraphobia
Third Year of Elementary School Fourth Year of Elementary School Fifth Year of Elementary School Sixth Year of Elementary School Total by factor |
6.38 9.25 7.96 6.68 7.61 |
9.00 11.17 8.50 8.00 8.94 |
3.75 7.33 7.11 5.73 6.20 |
0.250 0.438 0.742 0.469 0.020 |
|
Separation anxiety
|
9.38 9.00 8.91 7.84 8.66 |
9.75 10.00 10.00 10.13 10.00 |
9.00 8.00 7.22 6.18 7.23 |
0.854 0.094 0.164 0.031 0.001 |
|
Physical fears
Third Year of Elementary School Fourth Year of Elementary School Fifth Year of Elementary School Sixth Year of Elementary School Total by factor |
4.88 5.33 5.04 5.26 5.15 |
5.25 6.17 6.00 6.50 6.06 |
4.50 4.50 3.56 4.36 4.17 |
0.875 0.375 0.129 0.031 0.005 |
Analysis by anxiety levels
The results were obtained for the population in general and for factors with the purpose of establishing the levels of anxiety, according to the average scores (Table 2).
Table 2. Score of averages and equivalent percentiles by factor and gender, for the Spence test. The Total averages, both for girls and boys and in general, analyzed for each factor, was located in the levels of anxiety “Medium” and “Medium Low.” For the factors “Panic Attack and Agoraphobia,” “Separation Anxiety Disorder,” “Physical Fears,” as well as for the “General” average, it was determined that there was a significant difference with respect to gender
| Total (general) | Total (girls) | Total (boys) | Statistical difference by gender | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Factor = | Average | Percentile | Level of anxiety | Average | Percentile | Level of anxiety | Average | Percentile | Level of anxiety | Mann- Whitney Test (p =) | Signify | Tendency to |
| Panic Attack and Agoraphobia | 7.61 | 28 | Medium low | 8.94 | 33 | Medium low | 6.20 | 22 | Medium low | 0.020 | Significant | Girls |
| Separation Anxiety Disorder | 8.66 | 48 | MEDIUM | 10.00 | 55 | MEDIUM | 7.23 | 40 | Medium low | 0.001 | Very Significant | Girls |
| Social phobia | 8.11 | 45 | MEDIUM | 8.53 | 47 | MEDIUM | 7.67 | 42 | MEDIUM | 0.167 | NO Significant | |
| Physical Fears | 5.15 | 34 | Medium low | 6.06 | 40 | MEDIUM | 4.17 | 27 | Medium low | 0.005 | Very Significant | Girls |
| Obsessive- Compulsive Disorder | 7.63 | 42 | MEDIUM | 7.50 | 41 | MEDIUM | 7.77 | 43 | MEDIUM | 0.838 | NO Significant | |
| Generalized Anxiety Disorder | 8.90 | 49 | MEDIUM | 9.63 | 53 | MEDIUM | 8.13 | 45 | MEDIUM | 0.052 | NO Significant | |
| GENERAL | 46.06 | 40 | MEDIUM | 50.66 | 44 | MEDIUM | 41.17 | 36 | Medium low | 0.012 | Very Significant | Girls |
On the other hand, when performing Kruskal–Wallis analysis to find significant differences in anxiety levels for students, among the school grades analyzed (3rd, 4th, 5th, and 6th), for each factor (1-6) and by gender, no significant differences were found.
Child and adolescent depression questionnaire
Figure 2 presents the results of the CADQ test represented by the mean and the standard error considering the total population, totals by gender, and school grade. The group of fifth grade of the female sex obtained the lowest average with 10.93 points, while the group of third (male sex), the highest mean with 16.40. The third grade group holds the highest average with 16.4 but also re-presents the group with the most dispersed measures, which is due to the number of students that make up this group with n = 4. The average of the grand total (12.63) is located around the 12 points.
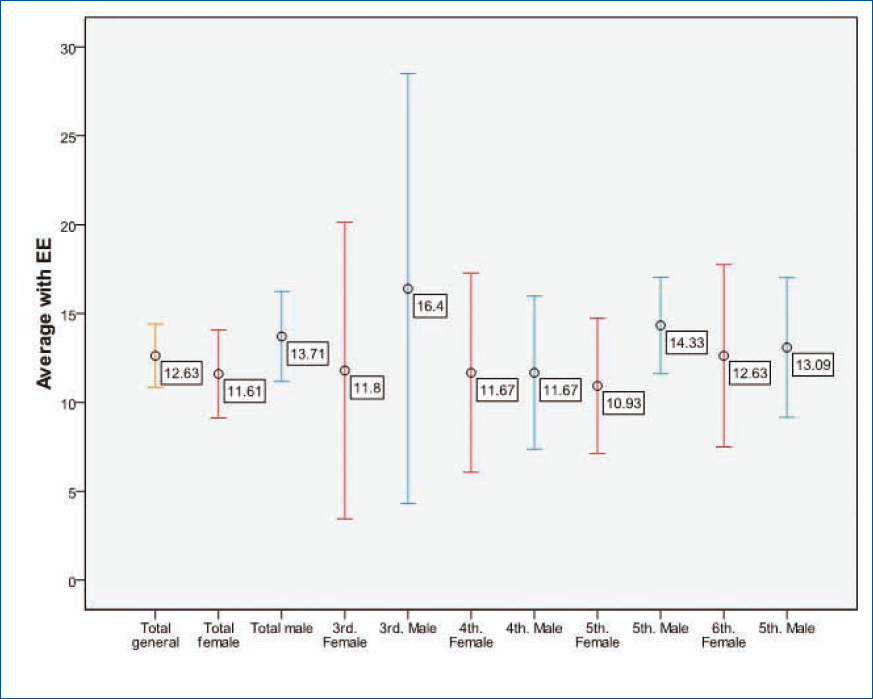
Figure 2. Standard error for the scores of Child and Adolescent Depression Questionnaire by global total, gender, and academic degree.
It can be identified that the averages of the CADQ test were always higher in the male subjects, except in fourth grade, where they are equal, this shows that children tend to score high for depression compared to girls (Fig. 2).
In the descriptive analysis, it was found that seven male and five female subjects had a score within the parameters for depression; this marks a tendency for male subjects to be more depressed than female subjects. We found 10 male and seven female subjects with indicators of psychological problems, while below 12 points (indicating absence of depressive or psychological problems), there were 14 male and 21 female. When performing the statistical analysis, no association was found between depressed subjects or with symptoms of psychological problems, and healthy subjects, in relation to gender (χ2 calculated: 2.2013 < 5.991).
In sixth grade, a greater number of cases were detected with depression scores (n = 5), while for psychological problems, the fifth grade reported more cases with n = 8. When performing the statistical analysis with χ2, it was shown that there is no association between depressed subjects, or with symptoms of psychological problems, and healthy subjects, with respect to the school grade (3rd-6th grade of primary school) (χ2 calculated: 4.34193 < 12.592).
Of the total (n = 62), 12 students achieved a score ≥ 19 in the CADQ test, equivalent to 19.35% with depressive symptoms, another 17 students obtained a score ≥ 12 and < 19 points, with a percentage of 27.42%, presenting symptoms of psychological problems, and 33 students presented a score < 12, with 53.23%, being considered without psychological or depressive problems.
Discussion
In our work, the measurements of anxiety and depression were made 1 month after the earthquake occurred, a condition that kept the population at that time in a critical situation regarding the degree of anxiety, insecurity, and panic. Gaeta-González and Pérez21, studied healthy Mexican children applying the scale of manifest anxiety in children/revised and the questionnaire of self-assessment anxiety state-trait in children. Their results show that in general girls score high compared to boys; fifth grade students show a significantly higher level of anxiety than those in sixth grade and in general, it stands out that in the last grades of primary education, there is a tendency to present significant levels of anxiety (medium, medium high, and high). Our post-earthquake assessments showed the following results: The sixth graders had a slightly higher anxiety score than the fifth graders, observing the same tendency mentioned by Gaeta-González and Pérez21, regarding the fact that in the last school grades, the tendency is to obtain a higher score for signs of anxiety (Table 1).
When comparing the analysis performed by percentile ranges, our results are similar to those of Gaeta-González and Pérez21 since in the category for the degree of anxiety, in most of the percentile ranges, it was “medium” and “medium low,” analyzed by each of the factors (Table 2). It should be noted that the study by Gaeta-González and Pérez21, was performed in healthy children without any previous factor, in our case the children were also healthy; however, they were evaluated a month after the earthquake occurred. It is possible that the similarity of our results compared with those of Gaeta-González and Pérez21, is due to the fact that the children evaluated only witnessed the earthquake and were not directly affected by it. Concerning to the depressive aspects, various percentages of depression due to earthquake have been reported in the literature. Thapa et al.22 showed that after 14 months of the Nepal earthquake in 2015, the prevalence of depressive symptoms was 8%. Farooqui et al.18 referred in his revision work some indexes of depression after an earthquake, for example, 25.98% of depression 2.5 years after the earthquake in Haiti, prevalence of 18.7% of major depression analyzed in a period of 3 years in Turkey, Goenjian et al.23 in the Armenian earthquake determined a correlation in terms of the presence of depression and the distance to the epicenter, so that at 75 km from the epicenter (low exposure area), there was an incidence of 28%, at 35 km from the epicenter (moderate exposure) 50% and in the epicenter (high exposure) 76% of cases. In our population studied 30 days after the earthquake, a percentage of 19.35% with depression scores was obtained in the students surveyed, with the epicenter located 120 km from Mexico City, affecting the south and center of the City. With respect to gender, there is a relationship with the aspects of anxiety and depression; the results of our study reveal with respect to anxiety that girls are more likely to suffer it, while depression is more common in boys (Table 2 and Fig. 2).
In the work of Gaeta-González and Pérez21, girls show a significantly higher level of anxiety with respect to children, according to our results (Table 1), which can be explained due to biological conditions, education and cultural aspects, and typical of the education in Mexico. In the study conducted by Eks¸i et al.24 children were more prone to suffer depression than girls, agreeing with the results obtained in our study (Fig. 2).
Farooqui et al.18 noted that women are at greater risk to trigger depressive and anxiety, in their work reports high percentages of anxiety with 63% and depressive symptoms with 54%, after an earthquake, coinciding with our work only in the aspects of anxiety, since the results of this work show that the male gender is more prone to develop depressive states, a condition that together with various factors can trigger a state of major depression that would lead to high suicide risks. Although in the exposed work, the objective is not directly related to the risk of suicide, it is important to point that in this type of work, follow-up must be given to those students who had high scores in the tests applied (CADQ test) since it is known that ideas and actions of suicide tend to increase as a result of earthquakes, in addition to being related to gender, the presence of anxiety and mainly depression25,26. As observed in the results, the levels of anxiety and depression that were obtained 30 days after the occurrence of the earthquake were not significant. For the future studies of this nature, they should be integrated into the evaluations of study, variables such as: The distance to the earthquake’s epicenter, the loss of a loved one, the direct presence of a traumatic event, and the parental situation, as well as the type of school the children attend (private or public). It is also important to consider the educational level, the information received through the media, and the preventive programs (seismic drills and alerts), aspects that may influence the evaluations of psychological disorders, to be clear about the origin of anxiety or depression presented by the study subjects.
Conclusions
This work demonstrates the importance of the culture prevention and attention to emergencies, with respect to situations generating to anxiety and depression, in traumatic and recurrent events in Mexico City, as in the case of earthquakes, a situation that can repeat in any urban area or densely populated city of the world, similar to Mexico City, considering this as the main contribution of this work. Since, in none of the tests (anxiety or depression) were significant indexes found in the evaluation of the elementary students surveyed in this study at 30 days after the earthquake, despite their proximity to sites with landslides, chaos, and loss of human lives. In addition, given the unprecedented situation of having performed a safety drill for earthquakes, a few hours before the earthquake of September 19, 2017, (with a magnitude of 7.1°and maximum acceleration of 58.83 cm/s2, according to data from the University National Autonomous of Mexico, we can affirm that this type of exercises, together with the protocols supervised by the National System of Civil Protection of Mexico, to offer prevention, aid, and recovery from disasters to the population, its goods and the environment, implemented in schools, workplaces, and public and private offices in the urban area, through the Civil Protection Brigades, would explain the results of low scores, both in anxiety (with “Low” and “Medium Low” levels), and with regard to depression, where it was observed that the majority of students (53.23% of the total) did not have a depressive state.
Funding
The authors declare that they have not received funding for this study.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical disclosures
Protection of humans and animals. The authors declare that the procedures followed conformed to the ethical standards of the committee for responsible human experimentation and in accordance with the World Medical Association and the Declaration of Helsinki.
Confidentiality of data. The authors declare that they have followed their center’s protocols on the publication of patient data.
Right to privacy and informed consent. The authors have obtained informed consent from the patients and/or subjects referred to in the article. This document is in the possession of the corresponding author.
Use of artificial intelligence to generate texts. The authors declare that they have not used any type of generative artificial intelligence in the writing of this manuscript or for the creation of figures, graphs, tables, or their corresponding captions or legends.
