Introduction
Awake fiberoptic intubation (AFOI) is the technique of choice for managing anticipated difficult airways, as it allows tracheal intubation in an awake, spontaneously breathing patient before induction of general anesthesia, thereby minimizing the risk of a “cannot intubate, cannot oxygenate” scenario1.
Successful awake intubation depends on proper patient selection, meticulous preparation, and a team familiar with the available techniques and airway planning strategies.
In this case report, we present the perioperative management of a 45-year-old female with a base of tongue tumor and severely limited mouth opening, scheduled for biopsy under general anesthesia. An awake tracheal intubation (ATI) approach was carefully planned and carried out using topical anesthesia, antisialogogue administration, intravenous (IV) sedation, and fiberoptic intubation (FOI). The procedure was completed successfully, without hemodynamic or respiratory complications, and was well tolerated by the patient.
When performed by an experienced team, AFOI remains a safe and effective technique in patients with anatomical complexities of the airway.
Case description
A 45-year-old woman, who provided consent for the reporting of this case, presented with a tumor at the base of the tongue and restricted oral aperture, scheduled for a biopsy. On admission, the patient reported a seven-day history of limited oral intake due to worsening oral symptoms and restricted mouth opening.
A tongue magnetic resonance imaging (Fig. 1) reported an infiltrative lesion is identified in the posterior two-thirds of the tongue, with irregular, poorly defined borders, predominantly involving the right half and crossing the midline. The lesion measures 42 × 32 × 43 mm in anteroposterior, transverse, and craniocaudal dimensions, respectively. No invasion of adjacent bone is observed.
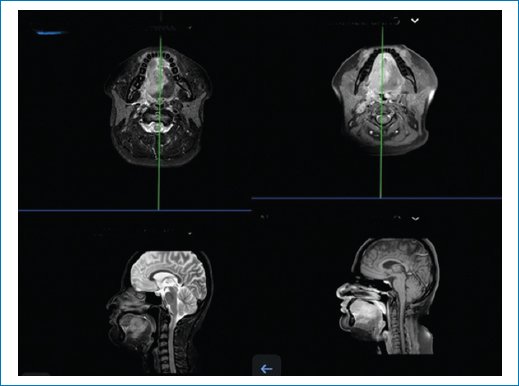
Figure 1. Pre-operative magnetic resonance imaging of the head and neck. Axial (top row) and sagittal (bottom row) T2-weighted images demonstrate an infiltrative lesion occupying the posterior two-thirds of the tongue, crossing the midline, and displacing adjacent oropharyngeal structures.
Ipsilateral lymphadenopathy is noted in level Ib (12 mm) and level IIa (14 mm) on the right side, both without central necrosis. Additional smaller lymph nodes with well-defined borders and homogeneous enhancement are present in levels Ib, IIa, IIb, and III.
The parotid and submandibular glands appear unremarkable. No abnormalities are observed in the nasopharynx, oropharynx, laryngeal structures, trachea, or cervical esophagus.
Diagnostic impression: infiltrative neoplasm involving the tongue and floor of mouth, associated with secondary nodal involvement, highly suggestive of squamous cell carcinoma.
The patient had no significant medical history. However, during the pre-operative evaluation, notable anatomical airway alterations were identified, including restricted oral aperture, an infiltrative neoplasm at the base of the tongue, increased pretracheal volume, limited neck extension, and restricted mandibular protrusion (Fig. 2).

Figure 2. Pre-operative and intraoperative preparation for awake fiberoptic intubation. A: pre-operative airway evaluation showing restricted mouth opening due to a posterior tongue mass. B: airway topicalization using a specialized atomization device for local anesthetic delivery, as part of the preparation for awake fiberoptic intubation. C: patient under monitored sedation with nasal oxygen supplementation before airway topicalization.
Given these anatomical challenges, a multidisciplinary team convened to discuss airway management strategies aimed at minimizing risks. ATI was selected as the preferred approach. The procedure was thoroughly explained to the patient, emphasizing clear, continuous communication throughout. The patient was instructed to raise her arm if she experienced discomfort, allowing for immediate adjustment or cessation of the procedure if necessary.
On arrival in the operating room, standard monitoring was initiated, revealing a blood pressure (BP) of 134/81 mmHg, heart rate (HR) of 86 bpm, and oxygen saturation (SpO2) of 99%. A dose of 500 mcg atropine IV was administered, and the patient was positioned at a 30° head-up angle with supplemental oxygen provided via a reservoir mask at 10 L/min. Nebulized lidocaine (80 mg) was started, and a dexmedetomidine infusion was administered at a rate of 0.5 μg/kg over 10 min. Additionally, a dose of 150 mcg fentanyl IV was administered.
Topical anesthesia was achieved with six sprays of 10% lidocaine on the anterior pillars of the oropharynx, followed by four sprays of 2% lidocaine. Lidocaine was applied to the tongue, oropharynx, and surrounding structures. When the patient no longer felt discomfort with a sputum suction tube, a Williams cannula was placed, and fiberoptic bronchoscopy was initiated shortly thereafter. On reaching the glottis, 2 mL of 2% lidocaine was administered through the bronchoscope’s working channel, achieving local anesthesia of the glottic and subglottic trachea. After a 2-min wait to ensure the anesthetic had taken effect, 2 mL of 2% lidocaine was again sprayed into the airway. The patient was instructed to cough gently, exposing the glottis, allowing the bronchoscope to pass smoothly through the glottis and reach the tracheal rings.
A 7.0 mm endotracheal tube (ETT) was then advanced over the bronchoscope without complications. Correct placement was confirmed by an end-tidal CO2 waveform, after which 50 mg of propofol IV was administered. Anesthesia was maintained with 2% sevoflurane and 7 cmH2O of pressure support ventilation. Vital signs remained stable throughout the procedure, with a BP of 115/75 mmHg, HR of 68 bpm, and SpO2 of 98%.
The surgery lasted approximately 25 min, and the patient was extubated fully awake without any complications.
Discussion
Awake intubation has become a fundamental skill in anesthesiologist training for managing complex airways. This technique offers significant advantages, including a strong safety profile by allowing spontaneous ventilation and maintaining airway tone until it is fully secured. Awake intubation has a low rate of complications and a high success rate, rarely requiring rescue strategies such as emergency surgical access. For these reasons, it is now considered the gold standard for anticipated difficult airway management and is incorporated into most complex airway management algorithms2,3.
Airway management in patients with oromaxillofacial tumors requires a multidisciplinary approach with advanced strategies. Patients can present restrict mouth opening, displace critical anatomical structures, and increase the risk of post-operative bleeding or edema. In oncology centers, approximately 25% of head and neck cancer patients undergo AFOI before a surgical or diagnostic procedure4.
According to the international guidelines from the Difficult Airway Society for ATI, there are four fundamental pillars for successful management: sedation, oxygenation, topicalization, and intubation. Various methods are described in the literature to achieve these essential components, and the choice of each strategy depends on the patient’s anatomical and physiological characteristics, available resources, and the operator’s experience1,5.
Furthermore, these guidelines recommend documenting awake intubation cases to inform and guide the management of future patients with similar pathologies. This documentation should include details on the oxygenation technique, topicalization method, sedation strategy, devices and tubes used, the intubation approach (nasal or oral), the number of attempts, and any adverse events or complications that may arise during the procedure6,7.
In line with these principles and the recommendations from international guidelines, we present a detailed account of our airway management strategy in this case. By systematically describing our choices regarding sedation, oxygenation, topicalization, and intubation, as well as the rationale behind each intervention, we aim to contribute to the clinical body of evidence and offer a reference for future cases with similar anatomical and procedural challenges. This approach not only reinforces the importance of individualized planning but also highlights key considerations that differentiate this case from others reported in the literature.
Preparation
The procedure was clearly explained to the patient, emphasizing the need for full cooperation to successfully secure the airway. We reassured the patient that communication would be maintained throughout, and we instructed her to raise her right hand at any time if she experienced pain, discomfort, or any other distress, allowing the anesthesia team to pause and address her needs as necessary. In anticipation of potential complications, we explicitly requested that the advanced airway cart be brought into the operating room and fully stocked. This cart includes a comprehensive set of airway management tools: supraglottic devices of various sizes, intubation adjuncts (such as stylets and bougies), different sizes of ETTs, adult and pediatric bronchoscopes, a manual jet ventilation system, and a complete cricothyrotomy and tracheostomy kit. Having immediate access to these resources is essential for rapid escalation if the primary intubation strategy fails or complications arise4.
In parallel, we optimized pharmacologic preparation with atropine to control secretions; we consider this to be a crucial aspect of AFOI, as excessive saliva can obstruct visualization and hinder bronchoscope maneuverability8.
At present, there is limited evidence and no general recommendations regarding the routine use of antisialogogues for awake intubation. However, vision during fiberoptic bronchoscopy can be enhanced with the use of antisialogogues, such as atropine, glycopyrrolate, or butylhyoscine. Some reports describe the use of intramuscular glycopyrrolate or atropine administered 40-60 min before intubation9,10.
Although glycopyrrolate is often favored in anesthesia due to its longer duration of action, minimal central nervous system effects, and more favorable cardiovascular profile, its IV formulation is not currently available in Mexico. As a result, we administered atropine, which is widely accessible, has a rapid onset, and remains an effective antisialagogue in this context. The decision was based on drug availability and the clinical need to minimize salivary secretions during FOI, while balancing the potential cardiovascular effects.
Secretions can have a significant impact on AFOI. We recommend optimizing salivary control as a key component of the anesthetic strategy when using a flexible bronchoscope.
Oxygenation
Since the patient had no prior pulmonary pathology, we decided to use nasal cannula at a flow rate of 5 L/min. In patients with underlying cardiopulmonary conditions, desaturation during the procedure may necessitate pausing and readjusting. In such cases, high-flow nasal cannula has been shown to be effective for this patient population. In addition, face masks with reservoir bags can be used to support oxygenation as needed8.
Sedation
The concept of an awake intubation is unpleasant and will frequently cause anxiety to patients. The goal of sedation is to create a patient who will be comfortable, cooperative, yet stable from a hemodynamic and respiratory standpoint. However, adverse effects of sedation can include hypoventilation, airway obstruction, oxygen desaturation, and cardiovascular instability. Consequently, selecting the right drug regimen is essential to ensure a safe and effective approach to ATI4,5.
There is no single optimal sedation technique for AFOI; rather, sedation must be tailored to the specific needs and conditions of each patient.
Commonly used medications include benzodiazepines such as midazolam, typically administered in anxiolytic doses (100-300 mcg/kg) are also typically combined with opioids like fentanyl or morphine. Early studies showed that high doses of midazolam without sufficient analgesia or topical anesthesia sometimes led to respiratory compromise and desaturation. While benzodiazepine-opioid combinations are accessible and familiar options for AFOI, their use requires careful dosing to prevent oversedation and associated respiratory risks11.
Some authors prefer dexmedetomidine, an alpha-2 agonist that provides sedation and anxiolysis without significant respiratory depression. Dexmedetomidine is generally infused with a loading dose of 0.5-1 mcg/kg over 10-20 min, followed by a maintenance infusion of 0.3-1.0 mcg/kg/h. It is important to monitor for cardiovascular effects, such as hypotension and bradycardia, which can occur with this administration9,12.
Fentanyl offers analgesia, cough suppression, and inhibition of airway reflexes, normally, it can be titrated with boluses of 25-50 mcg until the desired effect, adjusting the doses ensuring the patient remains awake, breathing, and cooperative throughout the procedure.
Recently, a systematic review and network meta-analysis on sedation techniques for ATI by El-Boghdadly et al. was published. The study evaluates various sedation regimens used to facilitate ATI, analyzing their effectiveness in terms of success rate, time to intubation, and risks of oxygen desaturation and cardiovascular complications. They compared 33 sedation regimens and included 2837 patients. They concluded that no single regimen proved superior success rates, but dexmedetomidine and ketamine were associated with reduced risks of oxygen desaturation. The authors emphasize that optimizing oxygenation, airway anesthesia, and procedural performance may be more influential than sedation choice, highlighting the need for individualized sedation strategies13.
A study by Mondal et al. suggests that a combination of dexmedetomidine and fentanyl provides better intubation conditions, adequate sedation, stable hemodynamics, and reduced desaturation during AFOI. In our patient, dexmedetomidine and fentanyl infusions provided excellent intubation conditions and stable hemodynamics throughout the procedure12.
Topicalization
Anesthetizing the upper airway can be achieved through several techniques, including the application of topical anesthetics (via sprays, solution sprayers, or nebulization) and the use of airway nerve blocks. Although there are numerous methods for achieving airway anesthesia, direct comparisons between them are limited. Nerve blocks are often preferred for AFOI because they deliver quick and profound anesthesia. Alternatively, nebulizing local anesthetics offers a promising approach, providing full airway anesthesia without the need for multiple, potentially painful injections.
The use of nerve blocks for airway anesthesia before awake intubation provides several advantages, including limiting the amount of sedation required and achieving a denser sensory blockade. Commonly employed nerve blocks include the superior laryngeal nerve block and the transtracheal block. The superior laryngeal nerve block, which can be performed using a landmark-based or ultrasound-guided approach, delivers local anesthetic near the thyrohyoid membrane. The transtracheal block anesthetizes the recurrent laryngeal nerve by delivering local anesthetic through the cricothyroid membrane.
Studies demonstrate that nerve blocks offer quicker time to intubation, higher-quality airway anesthesia, and improved patient comfort. While nebulization and topicalization techniques depend on delivery systems and may require more time to prepare and install3,14.
Some clinicians prefer a nebulization + topicalization technique, due to the ease of performance and lower risk of complications compared to nerve blocks. The maximum dose allowable for topicalization is less well established. The British Thoracic Society recommends 8.2 mg/kg/lidocaine. Other institutions recommend a lower limit of 4-5 mg/kg.
Intubation
In patients with limited oral aperture and distorted airway anatomy due to tumor infiltration, the use of a flexible fiberoptic bronchoscope becomes the most reliable and atraumatic method for securing the airway. In this case, videolaryngoscopy was not feasible due to restricted mouth opening (Mallampati IV, limited interincisor distance), and the insertion of a rigid laryngoscope could have resulted in failed exposure or tissue injury. A combined approach using videolaryngoscopy and fiberoptics was also ruled out for the same anatomical reasons. The Ovassapian airway was selected as a conduit because it facilitates midline advancement of the bronchoscope while protecting the oropharyngeal tissues and minimizing patient discomfort. It also ensures that the ETT can be delivered smoothly without impingement or resistance. This approach allowed for continuous oxygenation, optimal visualization, and first-pass success. Ultimately, the choice of device and intubation strategy should be tailored to the patient’s anatomical and clinical context to optimize safety and outcomes3,15,16.
Conclusion
This case highlights the critical importance of thorough pre-operative airway assessment and meticulous planning in patients with anticipated difficult airways due to base-of-tongue tumors. The successful management of this case underscores the need for a multidisciplinary approach, involving early collaboration between anesthesiologists and the surgical team to ensure a well-coordinated strategy.
The choice of AFOI (ATI) proved to be the safest and most effective technique in this scenario, allowing for controlled airway management while maintaining spontaneous ventilation. Adequate patient preparation, including optimized sedation, airway topicalization, and secretion control, played a key role in facilitating a smooth intubation process.
Furthermore, this case reinforces the importance of having a well-defined backup plan, including access to supraglottic airway devices, cricothyroidotomy kits, and surgical tracheostomy readiness in the event of failed intubation. Post-operative airway vigilance is equally crucial, as airway edema, hematoma formation, or delayed respiratory compromise can pose significant risks. Patients with severe airway obstruction may benefit from close observation, staged extubation strategies.
Ultimately, this case underscores the importance of a structured, patient-specific approach to complex airway management. The integration of advanced airway techniques, optimized sedation strategies, and patient communication and collaboration enhances patient safety and improves outcomes in complex cases of head and neck tumors.
Funding
The authors declare that they have not received funding.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical considerations
Protection of humans and animals. The authors declare that the procedures followed complied with the ethical standards of the responsible human experimentation committee and adhered to the World Medical Association and the Declaration of Helsinki. The procedures were approved by the institutional Ethics Committee.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from patients, and received approval from the Ethics Committee. The SAGER guidelines were followed according to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing of this manuscript.
