Introduction
Multifragmentary avulsion fractures of the inferior pole of the patella typically occur in young individuals and involve detachment of a portion of the patella, often with multiple fragments, due to excessive force exerted on the patellar tendon1. The patellar tendon is a strong fibrous structure that connects the patella to the tibia2. When subjected to excessive force, such as sudden deceleration or direct trauma to the knee, the patellar tendon may abruptly pull on the inferior pole of the patella, resulting in fracture. The severity of the fracture may vary, ranging from small avulsions to large multifragmentary detachments3.
Patients with inferior pole patellar fractures present with pain, swelling, loss of the knee extension mechanism, deformity, fluctuance, edema, and abrasions, among other findings.
Diagnosis is based on physical examination, in which discontinuity of the patellar tendon may be palpated, and on radiographs demonstrating the patellar fracture. Ultrasound (US) can visualize a fracture and/or discontinuity of the tendon. In some cases, computed tomography (CT) is required to assess the extent of the injury4.
Treatment of patellar tendon avulsion fractures is surgical in most cases in an effort to reinsert the tendon to the inferior surface of the patella and restoring the leg extension mechanism. Postoperatively, the knee is immobilized in extension with a brace or cast for 4 to 6 weeks3. After immobilization, initiation of physical therapy is essential to restore range of motion and strength5.
In the traditional technique, 3 tunnels are created using a 2.4- or 2.8-mm drill bit. A suture passer or guide is inserted through a tunnel from proximal to distal; once at the distal pole, the suture is introduced with the guide and passed proximally through the tunnels to perform a Krackow-type suture. This process may be complicated by poor visualization due to soft tissue, sometimes making it difficult to locate the tunnel and leading the surgeon to create a new one (it should be noted that the orthopedic surgeon should use the initial tunnels, as each additional tunnel increases the probability of refracture due to patellar weakening).
The objectives of this modified technique are to reduce operative time and facilitate passage of the sutures through the tunnels using the same instrument, thereby simplifying the surgical procedure.
Surgical technique
The patient is placed in the supine position with slight elevation of the ipsilateral gluteal region. With anesthesia previously agreed upon among the patient, surgeon, and anesthesiologist, prophylactic antibiotics are administered, followed by surgical site preparation and draping. Once the patient is ready, a surgical time-out is performed. A tourniquet may be inflated at the surgeon’s discretion.
The preferred approach is an anterior midline incision over the knee to visualize the extensor mechanism and identify and expose the fracture as well as the proximal end of the patellar tendon.
Figure 1 illustrates the surgical technique in 10 simple steps.
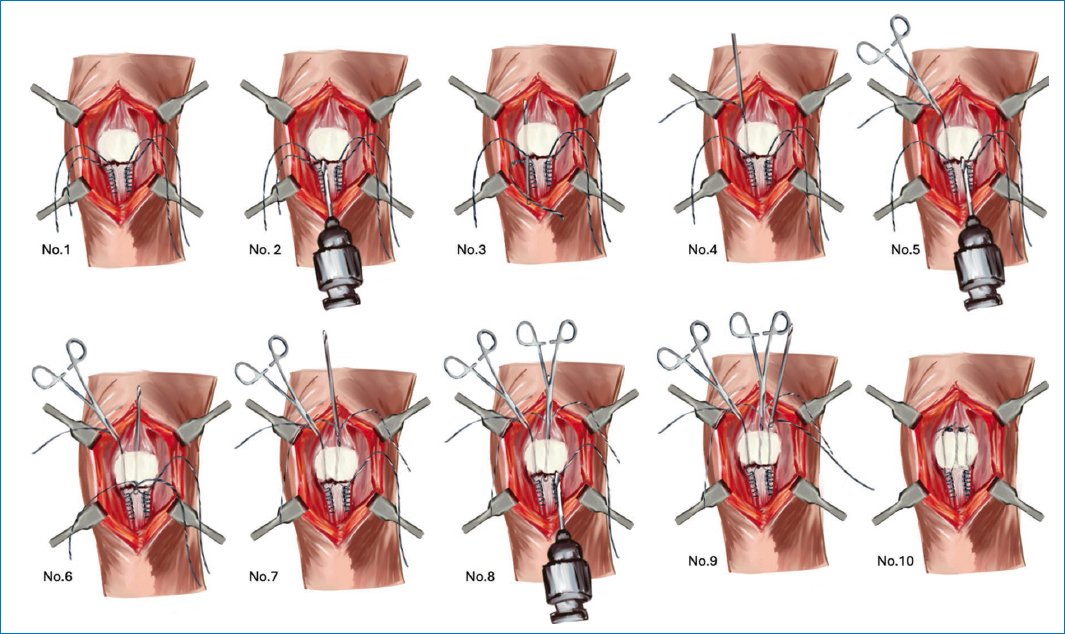
Figure 1. Description of the surgical technique.
Krackow-type stitches are placed at both ends (medial and lateral) of the tendon using nonabsorbable suture (in our case, braided polyester [TI-CRON] No. 5), leaving 4 long suture limbs at the proximal end of the tendon (No. 1).
Modification of the surgical technique
Using a 2.8-mm drill bit from the anterior cruciate ligament repair set (Arthrex) (Fig. 2), which has a cannulated distal end, a tunnel is created from distal to proximal toward the superior pole of the medial patellar surface (No. 2). Once the drill tip exits proximally, it is disconnected from the power source. The most medial suture limb is inserted into the distal cannulated end (No. 3), and the drill is pulled proximally to shuttle the suture through the tunnel (No. 4). Suture is, then, secured with a Kelly clamp to prevent it from slipping back through the tunnel.

Figure 2. 2.8-mm drill bit cannulated at the distal end.
A second tunnel is created in the midline of the patella (No. 5). In this case, 2 suture limbs are introduced: the lateral limb from the medial side and the medial limb from the lateral side (No. 6). They are pulled proximally (No. 7) and secured with a Kelly clamp.
Finally, a third tunnel is created in the lateral portion of the patella (No. 8), and the most lateral suture limb is passed through the cannulated drill (No. 9).
Return to the standard technique
Once all suture limbs have been passed to the superior pole of the patella, tendon reinsertion is performed by tensioning and tying medial to medial and lateral to lateral sutures (No. 10).
After reinsertion, correct anatomic patellar positioning, knee flexion-extension, and proper patellar tracking are verified. The excess suture is trimmed, the tourniquet is released if used, the wound is irrigated, hemostasis is achieved, and layered closure is performed. A hinged knee brace locked at 0° of extension is applied at the end of the procedure.
Expected outcomes
Postoperative outcomes and follow-up do not differ from the widely used technique. Knee flexion is restricted for at least 4 weeks. Thereafter, flexion is increased by 30° every 2 weeks under physical therapy supervision until 90° is achieved. After 2 weeks at 90° flexion, full flexion-extension is allowed with brace assistance for another 2 weeks. Subsequently, the brace may be discontinued and the patient allowed unrestricted ambulation.
Complications
One potential complication in both surgical techniques is drill bit breakage within the patella, preventing continuation of that tunnel and leaving a metallic foreign body in place. This complication is primarily related to drill wear; repeated use is not recommended.
Another complication, unrelated to the technique, is inadequate fibrosis at the tendon reinsertion site at the distal patellar pole.
Acknowledgments
The authors would like to thank to A. Woloski for support and design of the illustrations in figure 1 to clearly convey the surgical technique. Without this assistance, this would not have been possible, as clinical images alone do not convey each technical detail with the same clarity.
Funding
The authors declare that they have not received funding.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. This study does not involve personal data, medical records, or biological samples, and does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence.: The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
