Introduction
Ovarian cancer is the fifth most common neoplasm in women. The International Agency on Cancer reported 97 new cases in Mexico in 2020, between the ages of 0 and 19 years1. The ovary presents a wide range of malignant neoplasms, divided into epithelial cancer, germ cell tumors, stromal tumors of the sexual cords, and clinical carcinomas2. Germ cell tumors are the most common invasive cancers in children under 18 years (up to 50%) and those who had epithelial origin were 30 years of age (more than 90%)3. The etiology is unknown, but it is believed to be the cause of many cancers.
The etiology is unknown, but it originates from the surface of the ovarian epithelium or inclusion cysts. During ovulation, epithelial cells are internalized and damaged, and tissue repair mechanisms produce cells with an increased risk of mutation and neoplasia4.
The objective of this study was to identify the clinical characteristics of ovarian cancer in children under the age of 17 treated at a tertiary Hospital of Instituto Mexicano del Seguro Social in Puebla, México, from 2017 to 2023.
Methods
This is a descriptive, cross-sectional, ambispective study in a tertiary hospital of the Instituto Mexicano del Seguro Social in Puebla, Mexico.
We reviewed the records of patients with a diagnosis of ovarian cancer, aged 9-17 years, who were seen from 2017 to 2023. Patient records without a histopathology report or with incomplete information for any reason were excluded.
Clinical presentation, age at diagnosis, and histologic type were evaluated.
Descriptive statistics were used. Data were processed using the Statistical Package for the Social Sciences for IBM version 25.
This study was approved by the Health Research Committee 2101 of the Instituto Mexicano del Seguro Social (Registration R-2023-2101-030). Patient data were treated with strict confidentiality and used only for research purposes.
Results
We reviewed six patient files with a mean age of 16 years. The most common histopathologic diagnosis was dysgerminoma in 5 (83.3%) of the sample. One patient presented three histological types: Mucinous, borderline, and adenocarcinoma. Another patient had endometroid and dysgerminoma. The distribution according to the International Federation of Gynecology and Obstetric classification was early-stage IA (1), IB (3), IV1, and IIIA21 at the time of diagnosis.
The presence of a mass, pelvic pain, and abdominal distention was noted in 100% of the patients, and constipation in 4 (66.7%), dyspareunia, ascites, and amenorrhea were the least frequent features (Fig. 1).
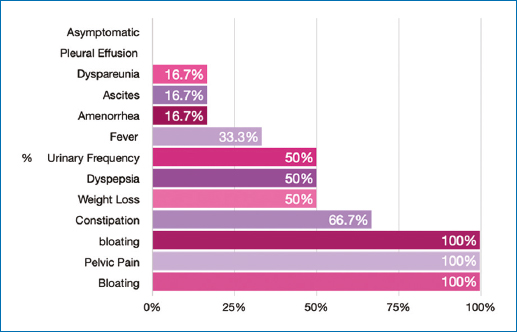
Figure 1. Clinical presentation.
Tumor markers were reported to be elevated in 4 patients (66.6%) and human gonadotropic hormone was elevated in 3 (50%) of the patients. The predominant surgical treatment was salpingo-oophorectomy plus omentectomy.
The frequency per affected ovary is shown in Fig. 2. Bilateral presentation was observed in 2 patients (33.3%).
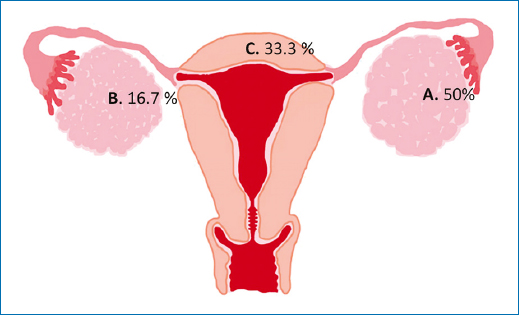
Figure 2. Frequency of affected organ. A: left ovary 50%; B: right ovary 16.7%, and C: bilateral ovary 33.3%.
It is also remarkable the case of a patient in whom ovarian cancer was an incidental diagnosis during her treatment for type B acute lymphoblastic leukemia. It was during her chemotherapy that she presented the symptomatology of pain, pelvic mass, and nocturnal fever.
Discussion
Ovarian cancer is one of the most common malignant neoplasms in women, and although it is not one of the main cancers in girls, its frequency is increasing5. It is estimated to have an incidence of 2.6 cases/100,000 children; and approximately 1% of all malignant pathologies in patients under 17 years6. Reports in Mexico are scarce and not recent. Therefore, this study aims to present the cumulative casuistry of ovarian cancer in children under 18 years in a tertiary public hospital from 2017 to 2023.
The most malignant types of tumors in pediatric population are germinal or stromal origin, compared to adults, which are epithelial type7. The Colegio Mexicano de Especialistas en Ginecología y Obstetricia (COMEGO) states that germ cell tumors represent 20-25% of ovarian tumors, mainly in girls and young women8. In this population, the highest frequency was recorded by dysgerminoma, with 35%.
The COMEGO and clinical practice guidelines state that all patients with suspected ovarian cancer should undergo basic laboratory tests, serum levels of the tumor marker CA-125, and office studies such as chest x-ray, pelvic ultrasound, and axial tomography9. Tumor markers do not confirm the diagnosis of ovarian cancer.
Tumor markers do not confirm the benignity or malignancy of the tumor, but they help to guide the diagnosis10. The most commonly used are α-fetoprotein, β-subunit of human chorionic gonadotropin, and lactate dehydrogenase. In this study, most of them were elevated11.
The definitive diagnosis requires histopathologic examination after surgical resection or by ultrasound-guided fine-needle biopsy10.
In a review of 6 years (1998-2004) in Mexican girls with ovarian neoplasms, the prevalence of malignant tumors was 34% of reported cases (16 cases), of which 56% were dysgerminomas12. Furthermore, in the present study, the most common histologic type was dysgerminoma (83.3%), and only two of the patients presented mixed type.
Ovarian dysgerminoma is one of the rarest malignant tumors in the general population. They are found at a relatively early stage with a more non-specific presentation in patients > 22 years. They originate from primary germ cells and are characterized by well-defined cells and abundant clear or eosinophilic granular cytoplasm rich in glycogen10,13. They spread in various routes (peritoneal seeding, intra-abdominal, and local extension) to adjacent structures such as the intestine, fallopian tubes, uterus, and bladder; by lymphatic route, they spread to lymph nodes, pelvic and retroperitoneal nodes14. Tumor cells can reach from the pelvis to the lower surface of the diaphragm, so large or small implants in the abdominal cavity are common15. No dissemination of primary tumors is reported in the present work.
Ascites and pleural effusion as a consequence of lymphatic obstruction16 occurred in only one case in this population.
The presentation of ovarian cancer is subacute, and what orients the diagnosis is the presence of a palpable abdominal and/or pelvic mass, dull abdominal pain, bleeding, rarely vaginal bleeding, and constipation10. The abdominal mass is usually solid, lobulated, with defined borders, located in the abdominopelvic cavity17. In the present series of cases, all patients presented these symptoms, with variable frequency.
Surgery plays an important role in the treatment of ovarian tumors as it helps in the diagnosis and staging of patients. A salpingo-oophorectomy is performed by laparotomy or laparoscopic approach11,18.
Surgery in these patients allowed staging and treatment at an early stage.
Multiple primary tumors are very rare. In this case series, two patients with two simultaneous primary tumors stand out; they are called synchronous if both ovaries are involved within a period of < 6 months, and metachronous if it is more than 6 months. The most common presentation is the ovarian-endometrial binomial19. Synchronous double primary tumors occur in 10% of ovarian cancer cases and 5% of endometrial cancer cases. The incidence of synchronous tumors in adults is 0.7%. In this study, it occurred in pediatric age and both ovaries, making it the only reported case of this type20.
Conclusion
Ovarian cancer in childhood has a low incidence. The most common symptoms are pelvic pain, bloating, and the presence of mass. The most common histological type is dysgerminoma.
Funding
The authors declare that they have not received funding.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article. Furthermore, they have acknowledged and followed the recommendations as per the SAGER guidelines depending on the type and nature of the study.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Use of artificial intelligence for generating text. The authors declare that they have not used any type of generative artificial intelligence for the writing of this manuscript nor for the creation of images, graphics, tables, or their corresponding captions.
