Introduction
Recurrent laryngeal papillomatosis (RLP) is the most common benign laryngeal neoplasm in adults. It is characterized by multiple proliferations of hyperplastic stratified squamous epithelium with a central fibrovascular core, and on the histopathology examination, it appears as a papillary tumor with a center of connective and vascular tissue1–3. It is caused by the human papillomavirus (HPV) and approximately 90% of cases by subtypes 6 and 11. HPV 11 is the most aggressive subtype, associated with recurrence, dissemination, and proliferation4–6. There are oncogenic genotypes, such as 16 and 18, which are involved in approximately 5% and have a probability of malignancy of 2%7–9.
RLP has an incidence of 1.8 for every 100,000 adults, with a low overall prevalence. The most common presentation is in males aged between 20 and 40 years old10,11.
There are two transmission routes: passing through the infected birth canal with HPV reactivation until adulthood and through sexual contact, specifically oral contact with infected genitals4,6. Risk factors include smoking, alcohol consumption, having multiple sexual partners, frequent practice of oral sex, and low socioeconomic status and educational level4,12. Most lesions are localized in the glottis, most commonly in the glottis, but there is evidence of extralaryngeal lesions6.
The most frequent clinical feature is dysphonia, leading to communication impairment and decreased quality of life. Other symptoms may include stridor and dyspnea13,14. Diagnosis is achieved through clinical examination and laryngeal endoscopy, with histopathological biopsy of the lesion as the gold standard. Clinical suspicion is often low, and diagnosis is often delayed2,15.
Treatment is symptomatic and not curative, leading to high morbidity due to recurrence13. Treatment options include adjuvant therapies (cidofovir and bevacizumab) and recurrent surgical resection of the lesions, with a high economic burden8,16. Prevention can be achieved using the nonavalent HPV vaccine (Gardasil® 9, Merck), but its limitation lies in population acceptance and adherence to the schedule17,18.
In Mexico, there is insufficient information on HPV typing in RLP. When diagnosed with an advanced clinical picture, recurrence and treatment failure are common. The highest prevalence is for types 6 and 11, while types 16, 18, 31, and 33 are rare. Therefore, knowing the frequency of HPV genotypes in Mexico allows for the prevention of aggressiveness, associated risk factors, and the final impact on the patient19,20.
The aim of this study was to type HPV genotypes in patients with RLP at a tertiary referral center from Puebla, Mexico.
Material and methods
This was a descriptive, cross-sectional study conducted on patients with RLP treated at a tertiary referral center from the Mexican Social Security Institute in Puebla, Mexico, over the past 3 years.
All patients seen in the unit with a diagnosis of RLP by biopsy of papillomatous lesions and confirmed by histopathology, older than 18 years, of any gender, and who signed informed consent were included. No patients were excluded.
Age, sex, presence of HPV, duration of evolution, the presence of diabetes mellitus, smoking status, and mode of birth (vaginal or C-section) were recorded. Clinical presentation, number of previous surgeries, location of lesions, age of sexual initiation, number of sexual partners, and practice of oral sex were also recorded.
Records were reviewed to collect the required information, and if necessary, patients were interviewed by phone to complete the data.
The presence of HPV was verified by polymerase chain reaction (PCR) using the following procedures: DNA extraction with the DNeasy® Blood and Tissue kit (Qiagen), HPV detection, and typing by PCR for genomes 6, 11, 16, and 18, using type-specific primer oligonucleotides.
The amplification reaction was performed using the PCR Master Mix kit (Promega), followed by agarose gel electrophoresis to determine the presence or absence of the genotype.
This protocol was approved by the local research committee No. 2101 of the Mexican Social Security Institute. All patients signed an informed consent form. Information was handled with strict confidentiality and used exclusively for research purposes.
Results
A total of 50 patients with a positive biopsy for HPV were recruited, 66% of whom were men and 34%, women. The mean age was 47.46 years, with a minimum age of 20 years, a maximum age of 90 years, and a standard deviation (SD) of 16.34; the most frequent age group was 41-50 years. The mean course of the disease was 2.7 years (SD, 1.07), most frequently 2 years.
A total of 26% of all patients were reported to have diabetes mellitus, 74% were smokers, and 70% were born vaginally. The most common clinical sign was stridor, occurring in 62% of cases. The mean number of previous surgeries was 2.02 (SD: 1.46), but up to 28% of patients underwent surgery four times; 24% had not been operated on. The mean age of sexual initiation was 16.12 years (SD: 2.06), with 38% reporting sexual initiation at 13-15 years old.
The mean number of sexual partners was 3.4 (SD: 1.04), with a predominance of 30% of the sample having 3 partners, and 78% reported practicing oral sex. Details are shown in table 1.
Table 1. Clinical variables of the patients with laryngeal papillomatosis
| n = 50 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 20-30 years | 31-40 years | 41-50 years | 51-60 years | 61-70 years | 71-80 years | > 80 years | |||
| 16% | 20% | 30% | 14% | 8% | 8% | 4% | ||||
| Birth mode | Vaginal | C-section | ||||||||
| 70% | 30% | |||||||||
| Age of sexual initiation | 13-15 years | 16-17 years | 18-19 years | |||||||
| 38% | 30% | 32% | ||||||||
| No. of sexual partners | 2 | 3 | 4 | 5 | ||||||
| 24% | 30% | 28% | 18% | |||||||
| Sexual partner | With oral sex | Without oral sex | ||||||||
| 78% | 22% | |||||||||
| Course of the disease | 1 year | 2 years | 3 years | 4 years | ||||||
| 14% | 34% | 20% | 32% | |||||||
| Clinical signs | Stridor | Respiratoy distress | ||||||||
| 62% | 56% | |||||||||
| Previous surgeries | 0 | 1 | 2 | 3 | 4 | |||||
| 24% | 14% | 16% | 28% | 18% | ||||||
HPV genotype 6 was identified in 62% of patients (Fig. 1), and the location was in the glottis in 94% (Fig. 2).
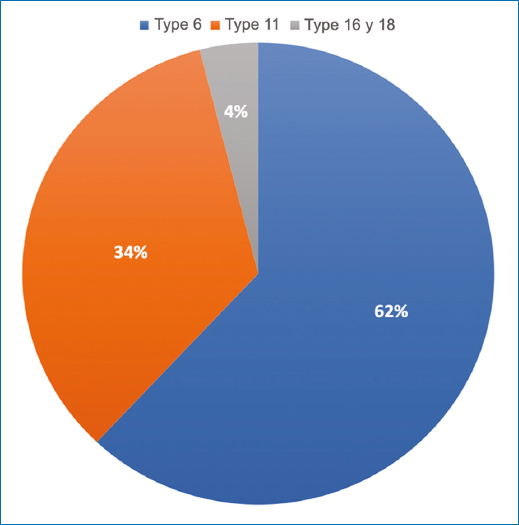
Figure 1. Prevalence of human papillomavirus genotypes identified.
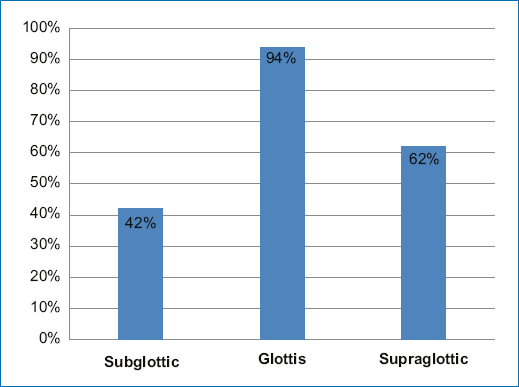
Figure 2. Anatomical location of recurrent laryngeal papillomatosis in the study patients.
Discussion
RLP is a serious, persistent, and unpredictable problem, with little tendency for malignancy, but it leads to physical and emotional sequelae with high medical costs. Its etiology is HPV, and the torpid evolution of the disease is related to the specific genotype6,11. This study identifies the most frequent HPV genotypes in the central-southern region of Mexico.
Male predominance is reported in up to 71% of cases21, which is consistent with this study (66%). Male frequency is associated with a higher number of androgen receptors in the vocal cords22.
Age, sexual initiation, and alcohol or tobacco consumption seem to be independent factors in the appearance of RLP; however, Freeman et al.23 concluded that smoking in patients with RLP increases the risk of malignancy. Literature also mentions factors that increase the risk of this disease, such as oral sex and having multiple sexual partners12, which is consistent with the findings made by this study, where 78% of patients practiced oral sex and up to 76% reported having 3 or more sexual partners.
Regarding transmission routes, vaginal delivery shows a greater risk of HPV exposure vs. C-section24. In our study, 70% of patients were born vaginally, which makes it difficult to establish a relationship between the mode of birth and RLP.
Another factor that can influence the frequency of RLP is diabetes mellitus due to being in a state of immunosuppression, as 26% of patients from this study were diabetic. However, different reports mention various conclusions found in this regard, so a greater understanding of each patient’s individual susceptibility is needed, considering whether it is due to intrinsic immune dysregulation or the presence of comorbidity25.
In different studies, the most common location is the glottis, as reported in the United States study conducted by Hu et al.9, who reported a prevalence of 84% for this location, which is consistent with our study, which reported a prevalence of 94%.
Regarding clinical presentation, dysphonia is mentioned as the most frequent symptom11,15. However, this study found a discrepancy with international literature, as stridor predominated in 62%.
We should mention that patients infected with genotype 11 require more frequent surgeries, shorter surgical intervals, and more adjuvant treatment. This has been reported in various studies, which mention means of 3 or more surgeries performed in these patients6,14; in this study, the mean is 3 surgeries. Repeated surgeries to remove papillomas induce squamous metaplasia of the ciliated epithelium, which increases the number of HPV infection subsites12.
In this study, HPV 6 is the most prevalent, reported in 62%, which is consistent with findings made in different international studies, such as in the one conducted by Japan by Yamada et al.14, while in Guadalajara, Jalisco, Mexico a predominance of genotype 16 was identified26. These discrepancies may be due to differences in the sensitivity of the method to detect different viral genotypes, as well as the integrity of the DNA of the samples analyzed26. In Mexico, there are few epidemiological studies on RLP, which is another factor that could explain the difference in the prevalence of genotypes. However, our study, despite having a small population sample size, yields results that are similar to those reported in the international literature in first-rate countries.
More studies with larger samples are needed to improve the statistical prevalence of HPV genotypes in RLP.
Conclusion
The study results allow us to conclude that, in cases of RLP in central-southern Mexico, the predominant HPV genotype is 6. Early initiation of sexual activity, having multiple sexual partners, and practicing oral sex are risk factors for developing RLP.
Funding
The authors declare that they have not received funding.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical responsibilities
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article. Furthermore, they have acknowledged and followed the recommendations as per the SAGER guidelines depending on the type and nature of the study.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Use of artificial intelligence for generating text. The authors declare that they have not used any type of generative artificial intelligence for the writing of this manuscript, nor for the creation of images, graphics, tables, or their corresponding captions.
