Introduction
Stereoelectroencephalography (SEEG) was first developed at Hospital Sainte-Anne of Paris, France for the first time back in 19491–3 (Fig. 1). Over the past decade, SEEG has been the method most widely used across the world to examine patients with focal epilepsy eligible for invasive epilepsy surgery. This migration from open surgery and placement of subdural grids through craniotomy requires epilepsy surgical centers to adapt their way of working, investment in surgical and imaging technology, and the comprehensive training of doctors involved in the SEEG program for the implantation of intracranial deep electrodes and proper interpretation of the registries4(Fig. 1).

Figure 1. First images of the SEEG system and early technology by Talairach and Bancaud.
The benefit of this extraordinary technology is that it allows us to carefully analyze anatomical-clinical-physiological correlations through a very precise intracranial multidimensional electrical registry. With these data, the spatial-temporal dynamics of the seizure can be studied. Also, it can be associated with its clinical expressions4 to establish a surgical plan. Within the first 25 years, this technique was only performed in Paris, France. Then, Switzerland, Canada, and the United States (2008). Back in 2018, epilepsy surgeons at Centro Neurológico del Centro Médico ABC started our SEEG program in Mexico. In this article we’ll be reviewing the very first case ever reported in Mexico of drug-resistant epilepsy (DRE) with electrode implantation followed by SEEG-guided radiofrequency thermocoagulation (SEEG-guided RF-TC) of the ictal onset zone. This jump started the SEEG era in our country.
On the days prior to implantation, a conceptual map was drawn based on a clinical, anatomical, and functional hypothesis for the placement of electrodes. Afterwards (Fig. 2A and 2B), a dedicated software and contrasted magnetic resonance imaging (MRI) for neuronavigation and an epilepsy protocol (HARNESS) were used. In addition, the trajectories of each electrode were planned, and a stereotactic (STX) implantation plan was implemented (Fig. 2).

Figure 2. A: Conceptual diagram to define the location of deep electrodes for SEEG. B: Screenshot of the working software used to define the stereotactic trajectories of each SEEG electrode on magnetic resonance.
The day of the surgery (day 0) the patient is taken to the computed tomography scan room and the STX system is placed conventionally (Zamorano-Dujovny) under local anesthesia. Afterwards, a contrasted computed tomography (CT) scan with STX protocol is performed and the patient is taken to the preoperative room while the STX halo is in position. Meanwhile, the CT scan images are fused with the implantation plan in a working station followed by trajectory correction to avoid vascular conflicts in the entire trajectory of each electrode. Then, the plan is reviewed and authorized by 2 neurosurgeons.
With the final plan, the patient is, then, taken to the operating room under balanced general anesthesia after asepsis, antisepsis, and placement of a sterile tissue with full doses of anticonvulsant drugs (ACD). Then, each of the electrodes previously selected for every trajectory is placed (PMT® of 4 to 18 contacts) starting with a triple verification while confirming the coordinates of each trajectory on the STX system followed by STX-guided 1 mm trephination (Fig. 3).

Figure 3. Skin puncture followed by STX-guided 1 mm trephination.
Afterwards, the dura mater is punctured with a dedicated punch, and the bolt is placed in the skull and SXT guided. The strength of the bolt is certified, and each electrode is gently inserted avoiding the outflow of cerebrospinal fluid and placing the external block screw (Fig. 4).
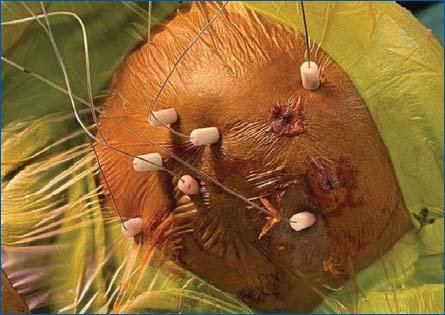
Figure 4. Final coupling with blocking screws of each SEEG electrode.
The proper placement is confirmed through fluoroscopy (through the O-Arm). Also, the proper functioning of each contact of the electrodes with support from intraoperative neurophysiology is checked.
After finishing the routine described for each electrode of the preestablished implantation plan, the patient is transferred for a follow-up CT scan (Fig. 5) and admitted to the intensive care unit on day 0. Form that moment onwards, the ongoing intracranial registry is started, and the maneuver activation protocol is implemented 3 to 4 times/day for as long as the entire registry lasts.

Figure 5. Immediate postoperative follow-up CT scan, and 3D reconstruction to confirm the lack of complications to have an anatomical idea of the final location of each SEEG electrode, thus allowing a better interpretation of the registry.
Starting on day 1, the patient is transferred to the intermediate care unit, and the gradual reduction of ACD is started to register seizures and interictal activity (Fig. 6). Based on the evolution and information obtained in the registry, it is decided what the best moment is to perform functional mapping with routines previously practiced with the neuropsychologist by applying cortical and subcortical electrical stimulation to record positive or negative responses (Fig. 6).

Figure 6. Example of a period of the ictal record in the monitoring unit in intermediate therapy.
Once the functional mapping has been completed and a large enough number of seizures has been registered to make a multidimensional map of the epileptogenic circuit, the epilepsy surgical team involved in SEEG (author and co-authors of this manuscript) is summoned. Afterwards, a multimodal diagram is drawn where all information obtained is added and schematized to decide on the definitive surgical treatment for each patient5.
Case presentation
The first case of SEEG-guided RF-TC is a 53-year-old man with a perinatal cerebral vascular event with right hemiparesis as a permanent side effect delaying motor development. The patient started with an early-onset seizure when he was 6 years old followed by a long 47-year history by the time of surgery. The patient is refractory to different well-selected ACD combinations and at the right doses with isolated peak interictal periods of 1 year with 2 to 3 seizures/week most often occurring during the day. Seizures start with an uncomfortable “ascending and descending sensation (the patient puts his hands on his chest to describe the feeling and then the throat). Then he shakes backwards. As a matter of fact, there are times that he sits down, which triggers accidental falls: he reports 1 consecutive week with several daily abdominal events. Also, he describes other events with the feeling that he is being “disconnected” and falls without any muscular tone. There are times when he shows dystonic moves with elevation of his right thoracic limb without loss of consciousness (not generalized seizures). The last generalized seizures happened when he was 14 or 15 years old in clusters of 2 to 3 back-to-back seizures in just a month. According to the definition established by the International League against Epilepsy of 20176, these are focal seizures without alteration of sensitive, focal motor (right thoracic limb), and emotional consciousness with occasional secondary generalization. The physical examination showed right hemiparesis of brachial and distal predominance of 3/5 and crural of 4-/5 with hyperreflexia and hypertonia, and right Babinksi sign. The cranial magnetic resonance imaging performed shows an extensive area of encephalomalacia of probable perinatal vascular etiology in angular, supramarginal, and left posterior-central gyrus with an area of perilesional gliosis (Fig. 7A). The functional MRI shows areas of rostral motor activation apart from the lesion (Fig. 7B). The ictal video-electroencephalogram shows electroclinical seizures with the typical onset semiology in electrode F2b2 (Fig. 8).

Figure 7. A: Extensive area of encephalomalacia probably of perinatal vascular etiology in angular and supramarginal gyrus and left posterior-central area with an area of perilesional gliosis. B: The functional magnetic resonance shows areas of rostral motor activation apart from the lesion.

Figure 8. A and B: SEEG-registered typical spontaneous electrical-clinical seizure. C and D: Seizure induced with electrical stimulation that evokes the typical semiology of spontaneous seizures. Note that both the spontaneous and the induced seizures have the same onset and progression pattern.
Results
Because he met the refractoriness criteria and due to the high load of seizures, his quality of life has deteriorated since his childhood, impacting negatively on his possibility of social, academic, and economic development. He comes to the ABC-Nacho epilepsy surgical program for vulnerable populations and with the support of the Amistad Clinic and altruistic families—after assessment by social workers—the patient is approved to undergo free-of-charge surgery at the ABC Medical Center in Santa Fe Campus, Mexico. The SEEG procedure was performed in June 22nd, 2022. Spontaneous and induced seizures are reported, and functional mapping is performed to study sensitivity, movement, and language through SEEG while the patient is awake in his room. The induced seizures were a very precise replica of spontaneous seizures (Fig. 8), which is, per se, a factor of good postoperative prognosis7.
The information is analyzed, and it is collectively decided that he is eligible for selective ablation through 1 of the SEEG electrodes implanted into the ictal onset site, and the SEEG-guided RFA is performed while the patient is awake and without pain. Afterwards, a follow-up CT scan is performed, and the patient is discharged the next day without morbidity (Fig. 9) after the electrodes are removed in the OR. Since the SEEG-guided RF-TC, the patient has had proper control of the seizures, is still on anticonvulsant medication and under neuropsychology and medical supervision. No epileptic seizures have been reported. However, there is clinical suspicion that non-epileptic paroxysmal events have occurred at the most recent follow-up (Fig. 9).

Figure 9. Confirmation of the site and size of the lesion obtained through SEEG-guided RF-TC, thus ruling out complications.
Discussion
The anticipated biological risk of experiencing, at least, 1 seizure during a person’s lifetime for the general population is 5% to 10%. One third of them will develop epilepsy. According to the World Health Organization, epilepsy accounts for 1% of morbidity load worldwide, more than breast cancer in women and almost as much as lung cancer in men8.
Drug-resistant epilepsy (DRE) is defined as the failure of the adequate trials of two schemes of tolerated drugs, chosen appropriately, and used (either in monotherapy or in combination) to achieve sustained absence of seizures. Successful treatment is the absence of seizures for one year or three times the previous interval among seizures. However, patients who experience seizures rarely should undergo a more prolonged follow-up before success can be determined9. DRE can be the source of cognitive, behavioral and psychiatric disorders, social problems for the patients and their caregivers, and a severe financial burden. It has a mortality rate (5 to 10 times higher compared to the general population), plus the risk of sudden death associated with epilepsy10. DRE has an incidence rate of 0.09/1000 people with recently diagnosed epilepsy and 9/1000 are eligible for epilepsy surgery11,12.
Despite informative campaigns and its proven safety and efficacy peofile, epilepsy surgery continues to be the most underused acceptable medical interventions. Early referral provides the best chances of preventing irreversible psychological and social problems, a life of disability and premature death8.
Minimally invasive techniques like SEEG and SEEG-guided RFA have become the safest techniques over the last two decades worldwide. Their indications are carefully studied, their efficacy has been well-established, and their use is accepted almost globally13–19.
After a period of almost 5 years of preparation, it has been possible to start the SEEG program in Mexico. Having successfully implanted the first deep intracranial electrodes through STX at the Neurological Center at Centro Médico ABC, our epilepsy surgical program center is defined as an advanced one. It is possible to use the SEEG technology in patients with DRE in a safe, precise, and efficient way to record the brain electric activity outside the OR for long periods of time (days) and while the patient is both asleep and awake, in the interictal and ictal periods, and to induce a seizure through cortical electric stimulation to confirm the ictal onset site and perform functional mapping while the patient remains awake and cooperative. The latter is particularly valuable, since transoperative functional mapping while patients are awake can be affected by the effect of the analgesic drugs used during the surgery early stage, which does not happen in SEEG mapping, since, in the second case, these are performed one or several days after implantation, outside the OR, and without the residual effects of analgesic drugs. Once information has been recorded and analyzed, it is possible to design a safe and effective surgical plan in most of the patients who have been adequatelt selected.
Conclusions
This is the very first case of SEEG and SEEG-guided RFA performed in Mexico. With the addition of this minimally invasive technique, a new technological era begins in which it is possible to explore, and offer surgical treatments to a group of patients with greater degree of complexity like patients with eloquent ictal onset sites, perisylvian, insular or deep areas with great safety and efficacy, which would have been impossible to study and treat otherwise. Despite the proven safety of this method, we should mention that this is an invasive diagnostic method (stage II) that should be performed at epilepsy surgical centers that have the appropriate technology and human capacity to do so adequately, both technically and ethically. The epilepsy surgical program at Centro Médico ABC has been implemented in an advanced epilepsy surgical center where these procedures are already performed on a routine basis while meeting the highest international standards. An early referral of people with DRE to specialized centers can improve the quality of life of individuals with epilepsy, as well as that of his family and social environment he/she is involved with, and reduce the risk of early death in this group of people.
Acknowledgement
We wish to thank the Gallardo Larrea, López-Dóriga Pérez Romo, Hagsater and Hojel families; members and social workers of the epilepsy surgical program at ABC-Nacho, Clínica Amistad, BRIMEX, Centro Médico ABC advisory board, Dr. Blanca Velázquez Hernández, Dr. Diana H. Martínez Castañeda, the directors and management of Centro Médico ABC, the OR staff, nurses, radiologists, intensive therapists, and all members from the epilepsy surgical program of Centro Médico ABC.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Funding
The authors declare that they have not received funding for this study.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
